

We’re supposed to believe that medical licensing exists to protect healthcare consumers from “quacks” and “charlatans.” The purpose, we’re told, is to improve the quality of healthcare, yet this system has manifestly failed to produce good patient outcomes.
The simple explanation for this is that medical licensing was never designed to protect the interests of healthcare consumers. Instead, the purpose has always been to protect the financial interests of a medical trade organization allied with the pharmaceutical industry. The effective result is a government-enforced medical cartel that masquerades as a “health care” system.
This explains the astronomical costs and disastrous health outcomes of so-called modern medicine, with alarming rates of chronic diseases among both the adult and childhood populations. An understanding of how and why medical licensing laws were established in the US is crucial for accurately diagnosing the symptoms of high costs and poor outcomes.
The AMA’s Medical Monopoly
Early in US history, various medical licensing laws were enacted to restrict the practice of medicine. The main beneficiaries of these laws were allopathic practitioners, while physicians who favored more natural and holistic approaches were marginalized.
We’re supposed to believe this was because consumers needed protection from “quacks,” but there was plenty of quackery to go around. Standard treatments within mainstream medicine included bloodletting, leeches, and administration of toxins like mercury and arsenic.
Unsurprisingly, consumers were dissatisfied with the outcomes and joined with alternative practitioners to demand freedom of choice. A successful movement arose to repeal medical licensing laws, and the early to mid-1800s became known as an era of “free trade in medicine.”
Medical schools abounded, there was a large supply of physicians, and market competition between different sects of physicians kept costs low while incentivizing innovation. The US had one of the healthiest populations in the world, with the lowest rate of infant mortality.
All that changed with the implementation of medical licensing. Disliking the competition, in 1847, allopathic practitioners organized to form the American Medical Association (AMA). From the start, the AMA’s goal was to establish a medical monopoly, and since it could never achieve that outcome through free market competition, it sought to have the government utilize force on its behalf.
The plan was to limit the number of medical schools, control the curriculum, and establish a licensing regime to restrict the practice of medicine to physicians adhering to the AMA-approved standard of care.
In 1891, the Journal of the American Medical Association (JAMA) boasted how effective the trade organization’s strategy had been in Illinois, where the state’s laws for regulating medical practice had succeeded in reducing the number of physicians.
The scarcely-concealed aim to impose a medical monopoly was thinly veiled in rhetoric about the need to protect consumers from themselves. The argument was that consumers were too ignorant and stupid to make right decisions about their own health, so—for their own good—they had to be denied the right of choice.
The US Supreme Court concurred. In the 1889 case Dent v. West Virginia, the Court upheld the conviction of a practitioner not for harming patients but for having obtained a degree from a college whose curriculum did not meet the approval of the state medical board. The courts consistently ruled that states had the authority to deny choice to consumers under their “police power”—and it served as no legal defense if the willingly-accepted treatments offered by alternative practitioners benefited their patients.
The AMA’s efforts to establish a medical monopoly were accelerated in the early 1900s through an alliance with other crony capitalists who offered even greater influence on government policymaking. A friend was found in the Rockefeller Institute—co-founded in 1870 by John D. Rockefeller—whose fortune was made in the petroleum industry—the chemical byproducts of which were used in the development of pharmaceutical drugs.
The Flexner Report
Because of its obvious conflict of interest, the AMA sought to conceal its role by approaching the Carnegie Foundation to commission a report that would evaluate medical schools and recommend curriculum. The head of the Carnegie Foundation was Henry S. Pritchett, who wrote in a memo to the head of the AMA’s Council on Medical Education, Arthur Bevan, MD,
When our report comes out, it is going to be ammunition in your hands. It is desirable, therefore, to maintain in the meantime a position which does not intimate an immediate connection between our two efforts.
Tasked with the job of producing the report was Abraham Flexner, who had no medical education, but whose brother Simon was head of the Rockefeller Institute for Medical Research. Published in 1910, the Flexner Report recommended that—to improve health care—most medical schools should be closed; medical boards should issue licenses only to graduates of AMA-accredited universities; and American taxpayers should subsidize the remaining schools and their approach to medical research.
The report’s recommendations were widely implemented, resulting in a precipitous decline in the number of healing schools. Minorities were disproportionately harmed. Of the seven medical schools in the country for African Americans, Flexner recommended keeping just two. (In 2008, the AMA formally apologized for “its past history of racial inequality toward African-American physicians”).
In 1913, Flexner was rewarded for his service with the position of Secretary to the Rockefeller Foundation’s General Education Board. Founded that same year, the Rockefeller family’s new “philanthropic” foundation sought to steer the direction of medical research and education in favor of pharmaceutical treatments, funding Johns Hopkins University and other drug-medicine schools whose approach incorporated the scientific method.
The financial agenda of the alliance between the AMA and nascent pharmaceutical industry was thus masked under the guise of advancing “medical science,” and mainstream historical accounts credit the Flexner Report with advancing evidence-based medicine. However, educational reform toward more scientific approaches in medicine was already underway. The Flexner Report didn’t create that movement but hijacked it.
By narrowly controlling the direction of medical research according to an institutionalized bias, the monopolistic system advanced by the report has done more to retard than to advance health care. One must consider the opportunity cost of how funding for medical research might otherwise have been put to better use, had the direction of resources been allowed to be determined by the pricing system of a competitive market.
Indeed, because of the government’s special treatment of the AMA, the very practice of “medical science” has been deeply corrupted, with inherent conflicts of interest aligned with the financial interests of the pharmaceutical industry. The result has been a myopic focus on treating symptoms with drugs instead of addressing root causes.
The resulting medical paradigm conceptualized the body in terms of systems unrelated to each other. Diagnostics and therapies were developed on the premise that you could treat one system without affecting the rest of the body. More natural and holistic approaches to health care and maintenance were marginalized.
Claiming Undeserved Credit
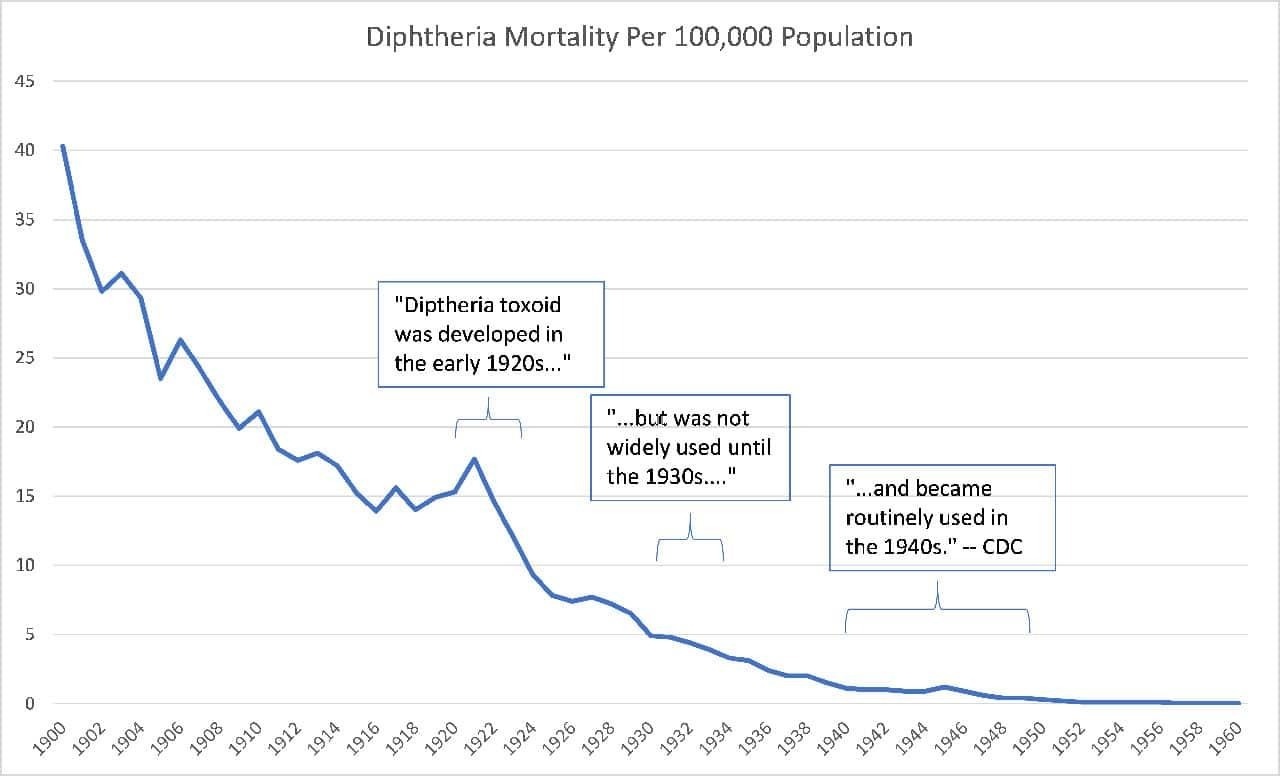
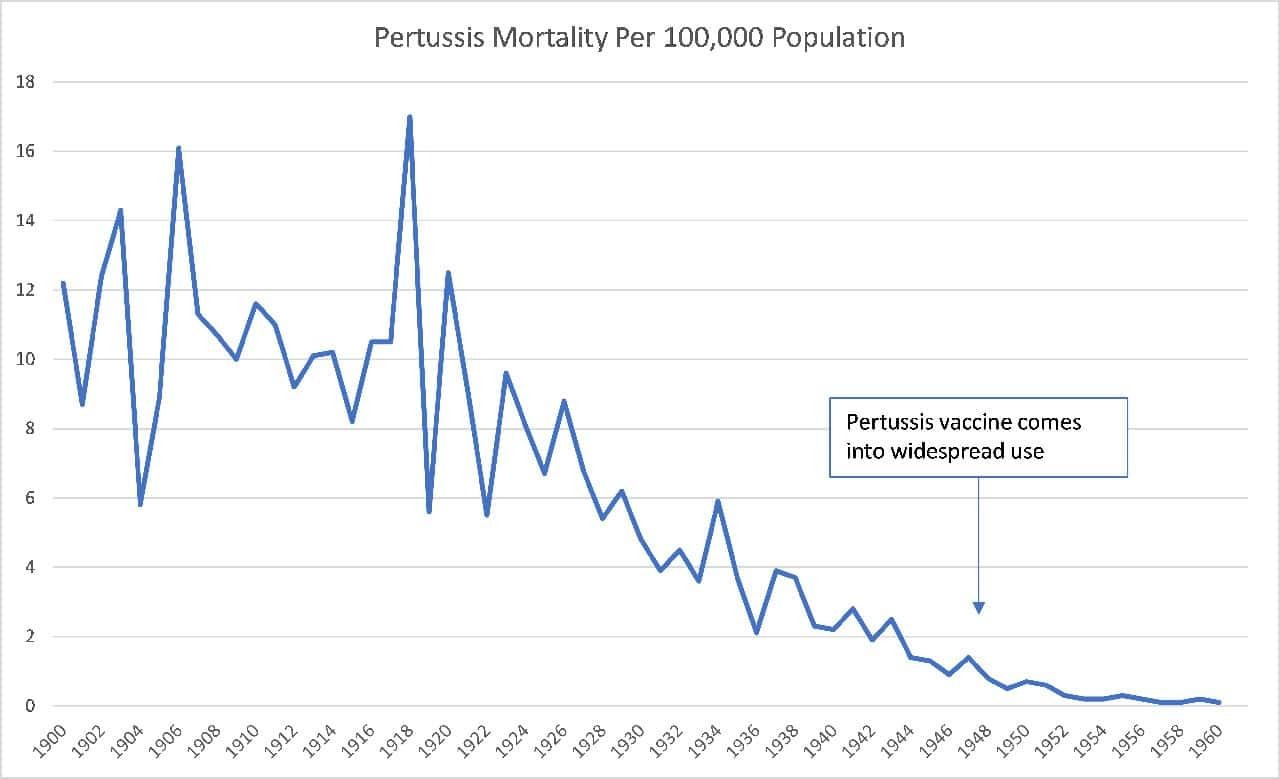
Another myth constantly reinforced by the medical cartel is that its therapeutic measures were responsible for the dramatic decline in mortality observed during the twentieth century. Most specifically, we are supposed to believe that vaccines were the cause of dramatic reductions in infectious disease mortality, but it is a simple fact of the historical data that these reductions mostly occurred before there were even any vaccines to possibly help explain it.
Here, for example, is the data for diphtheria:
Here’s pertussis:
And here’s the dreaded measles:
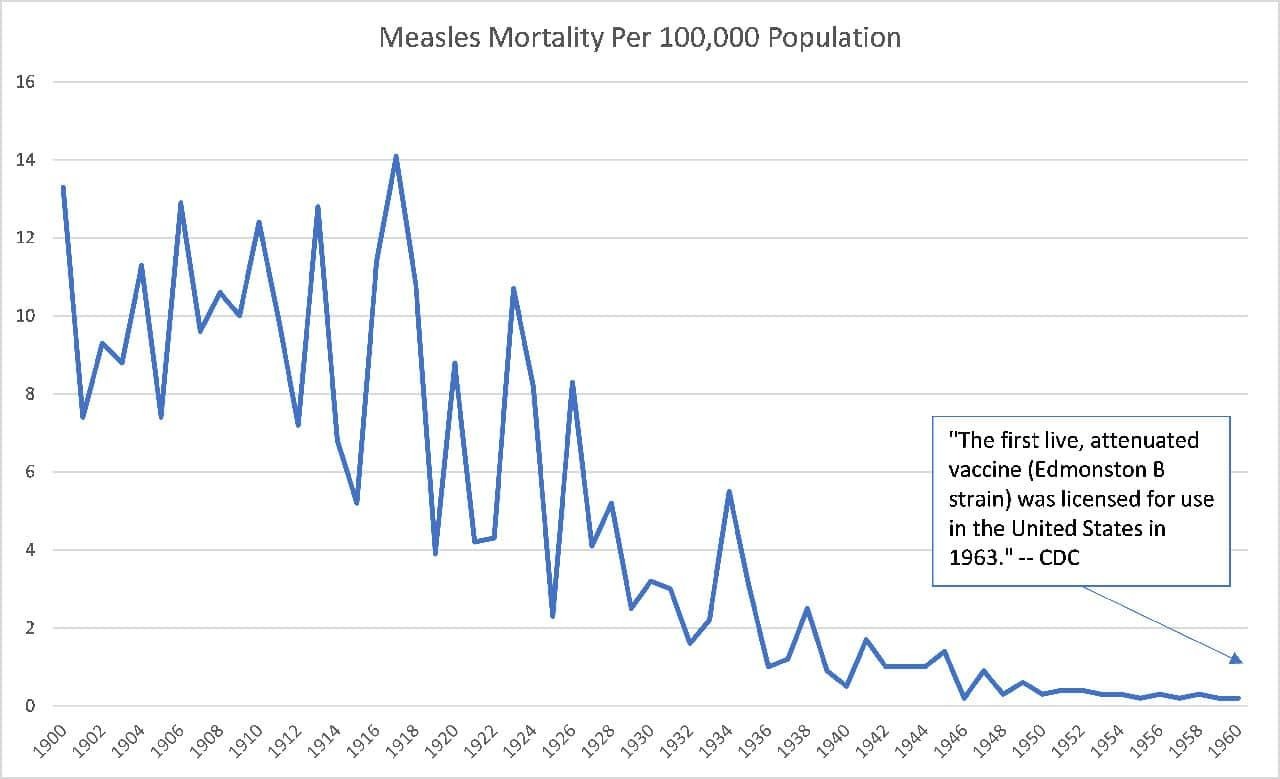
These dramatic reductions in disease mortality were instead due to factors related to an increasing standard of living, including sanitation, refrigeration, less crowding, better personal hygiene, and better nutrition.
It’s a myth that “modern medicine”—including the practice of coerced mass vaccination—is “evidence-based.” This is a legend that we are told to manufacture our consent for the pharma-centric medical cartel that masquerades as a health care system.
The AMA and its partners in crime succeeded greatly in perverting medical science to suit their financial agenda, accomplished by eliminating free market competition, reducing the supply of physicians, and helping to drive health care costs up to where they are today.
The War on Informed Consent
It is important to understand how the regime of medical licensing violates fundamental human rights. As illustrated by the case study I present in my book The War on Informed Consent, licensing is weaponized against ethical physicians who respect parents’ right to make their own informed choices about childhood vaccination.
In that case, Dr. Paul Thomas—a pediatrician practicing in Oregon—posed a threat not to public health but to the so-called “public health” establishment. Whereas the state’s policy goal was to achieve a high vaccination rate, Dr. Thomas’s goal was to produce a healthy patient population. A peer-reviewed analysis of his patient data proved that his approach was working, which prompted the state medical board to emergently suspend his license.
Besides the systematic violation of the right to informed consent, the licensing regime violates the right to contract and personal autonomy. Individuals have a right to decide for themselves whom they see for health care and what services they’d like to pay for, and this right is violated by the restrictions that licensing places on consumer choice.
Individuals also have a right to make decisions about their own bodies, without the government dictating what those choices ought to be. The idea that licensing ensures higher quality of care is seriously challenged by empirical observation. The real consequences of medical licensure include a loss of consumer choice—an artificially-restricted supply of physicians, increased costs for health care, stagnated medical research, and alarmingly-poor health outcomes.
Indeed, licensure criteria are based on acquisition of knowledge about how to diagnose and treat within the confines of established “standard of care,” not on clinical performance. Being able to pass tests in medical school and obtain a license from a state board does not translate into a healthy population.
Conclusion
Simply stated, the medical cartel’s education system is designed to limit the supply of physicians to only regime-approved trainees—not to improve patient outcomes. The conclusion that medical licensing should be abolished might sound radical to most Americans, but it shouldn’t. It’s not as though there wouldn’t remain standards of education, accreditation, and certification. All of these are already provided by the market and would continue to exist in the absence of state licensing boards, which are a perverse anachronism from an age of medical barbarism.
It’s also not as though consumers wouldn’t be able to discern between practitioners whose patients get better and those whose don’t. One doesn’t need a medical degree to tell the difference in health outcomes.
Healthcare consumers do not need to be protected from themselves; they need to be protected from the government-enforced medical cartel that has caused such a catastrophe in both costs and outcomes.
The correct diagnosis for the symptoms of unaffordable care and a sick population is the disease of medical licensing. The treatment to destroy this cancer is simple: get the government out of the business of our health.
This is a condensed summary of an in-depth report on the history of medical licensing and its consequences. For the full details and documentation, read “Why Medical Licensing Should Be Abolished.”

